Focused Trauma Conference 2017: Deel Drie
In the third part of the day we focused on balloons, namely REBOA (Resuscitative Endovascular Balloon Occlusion of the Aorta) - the Life in the Fast Lane post can be found here. The talk was by @emeddoc. This procedure is intended for cases of non-compressible traumatic haemorrhage. Before REBOA the best possible method to achieve haemostasis was through compressing the descending aorta via resuscitative thoracotomy (RT). Data from the American Association for the Surgery of Trauma (AAST) in 2014 shows that REBOA is at least non-inferior to RT. In trauma patients in LOST (ie not TCA yet) who required REBOA 92.6% survived their stay in ED and 22.2% survived to discharge. Increasingly work has shown REBOA to be feasible in the pre-hospital setting and has the best survival rates if performed pre-hospital.
However, a study from Japan showed that REBOA is associated with an increase of 16.5% in mortality. However, the median door to surgery time was 97 minutes and further research has shown in animal studies that lactate clearance is intact 45-60 minutes post REBOA but after that the ischaemia distal to the balloon may be irreparable hence the poor date from Japan. This raises the possible of future research into partial inflation to not completely cut off distal flow and have some permissive hypotension.
REBOA is not just for the pre-hospital medics to be concerned about; it requires clear handover to the hospital and theatre teams after it is used as it will alter physiology. It it there to buy time for the definitive surgery and it was emphasised several times that any unit wanting to implement REBOA will require widespread organisation and culture change.
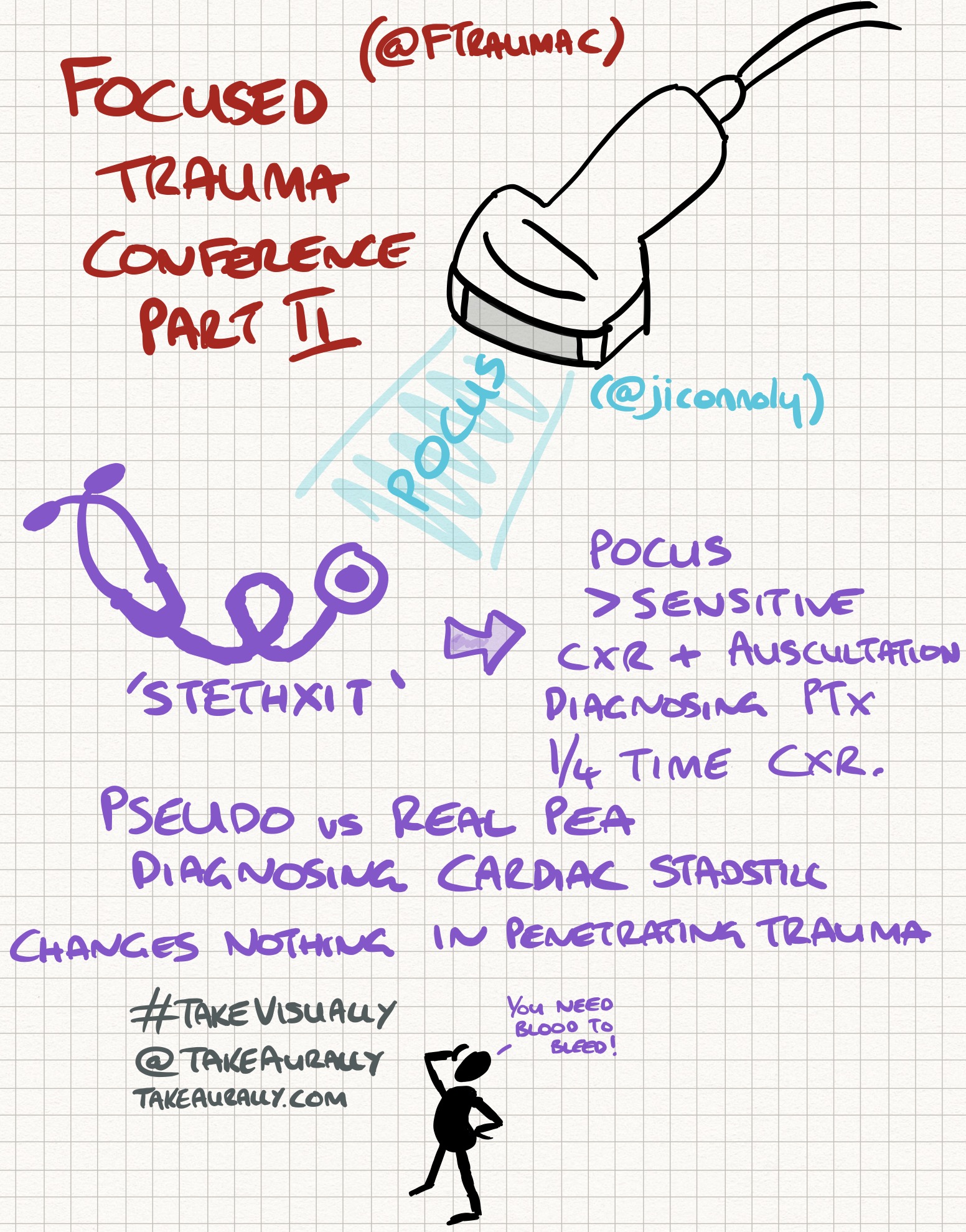
Here is the Take Visually graphic for this podcast and blog:
It was a brilliant and interesting day; thank you to all the organisers. Antwerp is a lovely city and the Belgian people were very welcoming; if you can visit do!